Stages of Birth
First stage: dilationThere are several factors that midwives and physicians use to assess the laboring mother's progress, and these are defined by the Bishop Score. The Bishop score is also used as a means to predict whether the mother is likely to spontaneously progress into second stage (delivery).
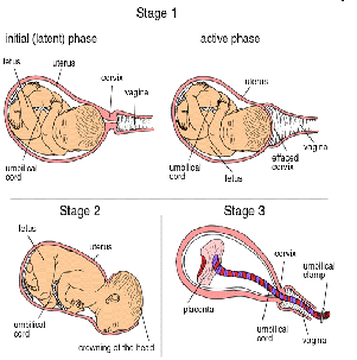
The first stage of labor starts classically when the effaced (thinned) cervix is 3 cm dilated. There is a variation in this point as some women may or may not have active contractions prior to reaching this point. The onset of actual labor is defined when the cervix begins to progressively dilate. Rupture of the membranes, or a blood stained 'show' may or may not occur at or around this stage.
Uterine muscles form opposing spirals from the top of the upper segment of the uterus to its junction with the lower segment. During effacement, the cervix becomes incorporated into the lower segment of the uterus. During a contraction, these muscles contract causing shortening of the upper segment and drawing upwards of the lower segment, in a gradual expulsive motion. The presenting fetal part then is permitted to descend. Full dilation is reached when the cervix has widened enough to allow passage of the baby's head, around 10 cm dilation for a term baby.
The duration of labour varies widely, but active phase averages some 20 hours for women giving birth to their first child ("primiparae") and 8 hours[citation needed] for women who have already given birth ("multiparae"). Active phase arrest is defined as in a primigravid woman as the failure of the cervix to dilate at a rate of 1.2 cm/hr over a period of at least two hours. This definition is based on Friedman's Curve, which plots the typical rate of cervical dilation and fetal descent during active labor. Some practitioners may diagnose "Failure to Progress", and consequently, perform a Cesarean.
Second stage: fetal expulsionThis stage begins when the cervix is fully dilated, and ends when the baby is born. As pressure on the cervix increases, the Ferguson reflex increases uterine contractions so that the second stage can go ahead[citation needed]. At the beginning of the normal second stage, the head is fully engaged in the pelvis; the widest diameter of the head has passed below the level of the pelvic inlet. The fetal head then continues descent into the pelvis, below the pubic arch and out through the vaginal introitus. This is assisted by the additional maternal efforts of "bearing down" or pushing. The fetal head is seen to 'crown' as the labia part. At this point, the woman may feel a burning or stinging sensation.
Complete expulsion of the baby signals the successful completion of the second stage of labor.
A newborn baby with umbilical cordready to be clamped. The second stage of birth will vary by factors including parity, fetal size, anesthesia, the presence of infection. Longer labors are associated with declining rates of spontaneous vaginal delivery and increasing rates of infection, perineal laceration, obstetric hemorrhage, as well as need for intensive care of the neonate Third stage: umbilical cord closure and placental expulsionFurther information: Umbilical cord and Placental expulsionBreastfeeding during and after the third stage, the placenta is visible in the bowl to the right.The period from just after the fetus is expelled until just after the placenta is expelled is called the third stage of labor.
The umbilical cord is routinely clamped and cut in this stage, but it would normally close naturally even if not clamped. A 2008 Cochrane Review looked into the timing of clamping the umbilical cord. It found that the time of clamping made no difference to the mother, but did have effects for the baby. If the cord is clamped after 1–3 minutes, the infant receives increased amounts of haemoglobin in their first months of life, but may have an increased risk of needing phototherapy to treat jaundice. Sometimes a newborn’s liver is slow to break down all of the red cells they had in the womb, particularly if they are left with more fetal blood from delayed cord clamping and phototherapy helps to speed the breakdown.
Placental expulsion begins as a physiological separation from the wall of the uterus. The period from just after the fetus is expelled until just after the placenta is expelled is called the third stage of labor. The average time from delivery of the baby until complete expulsion of the placenta is estimated to be 10–12 minutes dependent on whether active or expectant management is employed
Placental expulsion can be managed actively, by giving a uterotonic such as oxytocin along with appropriate cord traction and fundal massage to assist in delivering the placenta by a skilled birth attendant. Alternatively, it can be managed expectantly, allowing the placenta to be expelled without medical assistance. In a joint statement, World Health Organization, the International Federation of Gynaecologists and Obstetricians and the International Confederations of Midwives recommend active management of the third stage in all vaginal deliveries. This is a strong recommendation of theWorld Health Organization backed by moderate base evidence citing reduced risk of postpartum bleeding (i.e.: obstetric hemorrhage).
In as many as 3% of all vaginal deliveries, the duration of the third stage is longer than 30 minutes and raises concern for retained placenta.
When the amniotic sac has not ruptured during labour or pushing, the infant can be born with the membranes intact. This is referred to as "being born in the caul." The caul is harmless and its membranes are easily broken and wiped away. With the advent of modern interventive obstetrics, artificial rupture of the membranes has become common, so babies are rarely born in the caul.Fourth stageThe "fourth stage of labor" is a term used in two different senses:
The first stage of labor starts classically when the effaced (thinned) cervix is 3 cm dilated. There is a variation in this point as some women may or may not have active contractions prior to reaching this point. The onset of actual labor is defined when the cervix begins to progressively dilate. Rupture of the membranes, or a blood stained 'show' may or may not occur at or around this stage.
Uterine muscles form opposing spirals from the top of the upper segment of the uterus to its junction with the lower segment. During effacement, the cervix becomes incorporated into the lower segment of the uterus. During a contraction, these muscles contract causing shortening of the upper segment and drawing upwards of the lower segment, in a gradual expulsive motion. The presenting fetal part then is permitted to descend. Full dilation is reached when the cervix has widened enough to allow passage of the baby's head, around 10 cm dilation for a term baby.
The duration of labour varies widely, but active phase averages some 20 hours for women giving birth to their first child ("primiparae") and 8 hours[citation needed] for women who have already given birth ("multiparae"). Active phase arrest is defined as in a primigravid woman as the failure of the cervix to dilate at a rate of 1.2 cm/hr over a period of at least two hours. This definition is based on Friedman's Curve, which plots the typical rate of cervical dilation and fetal descent during active labor. Some practitioners may diagnose "Failure to Progress", and consequently, perform a Cesarean.
Second stage: fetal expulsionThis stage begins when the cervix is fully dilated, and ends when the baby is born. As pressure on the cervix increases, the Ferguson reflex increases uterine contractions so that the second stage can go ahead[citation needed]. At the beginning of the normal second stage, the head is fully engaged in the pelvis; the widest diameter of the head has passed below the level of the pelvic inlet. The fetal head then continues descent into the pelvis, below the pubic arch and out through the vaginal introitus. This is assisted by the additional maternal efforts of "bearing down" or pushing. The fetal head is seen to 'crown' as the labia part. At this point, the woman may feel a burning or stinging sensation.
Complete expulsion of the baby signals the successful completion of the second stage of labor.
A newborn baby with umbilical cordready to be clamped. The second stage of birth will vary by factors including parity, fetal size, anesthesia, the presence of infection. Longer labors are associated with declining rates of spontaneous vaginal delivery and increasing rates of infection, perineal laceration, obstetric hemorrhage, as well as need for intensive care of the neonate Third stage: umbilical cord closure and placental expulsionFurther information: Umbilical cord and Placental expulsionBreastfeeding during and after the third stage, the placenta is visible in the bowl to the right.The period from just after the fetus is expelled until just after the placenta is expelled is called the third stage of labor.
The umbilical cord is routinely clamped and cut in this stage, but it would normally close naturally even if not clamped. A 2008 Cochrane Review looked into the timing of clamping the umbilical cord. It found that the time of clamping made no difference to the mother, but did have effects for the baby. If the cord is clamped after 1–3 minutes, the infant receives increased amounts of haemoglobin in their first months of life, but may have an increased risk of needing phototherapy to treat jaundice. Sometimes a newborn’s liver is slow to break down all of the red cells they had in the womb, particularly if they are left with more fetal blood from delayed cord clamping and phototherapy helps to speed the breakdown.
Placental expulsion begins as a physiological separation from the wall of the uterus. The period from just after the fetus is expelled until just after the placenta is expelled is called the third stage of labor. The average time from delivery of the baby until complete expulsion of the placenta is estimated to be 10–12 minutes dependent on whether active or expectant management is employed
Placental expulsion can be managed actively, by giving a uterotonic such as oxytocin along with appropriate cord traction and fundal massage to assist in delivering the placenta by a skilled birth attendant. Alternatively, it can be managed expectantly, allowing the placenta to be expelled without medical assistance. In a joint statement, World Health Organization, the International Federation of Gynaecologists and Obstetricians and the International Confederations of Midwives recommend active management of the third stage in all vaginal deliveries. This is a strong recommendation of theWorld Health Organization backed by moderate base evidence citing reduced risk of postpartum bleeding (i.e.: obstetric hemorrhage).
In as many as 3% of all vaginal deliveries, the duration of the third stage is longer than 30 minutes and raises concern for retained placenta.
When the amniotic sac has not ruptured during labour or pushing, the infant can be born with the membranes intact. This is referred to as "being born in the caul." The caul is harmless and its membranes are easily broken and wiped away. With the advent of modern interventive obstetrics, artificial rupture of the membranes has become common, so babies are rarely born in the caul.Fourth stageThe "fourth stage of labor" is a term used in two different senses:
- It can refer to the immediate puerperium, or the hours immediately after delivery of the placenta.
- It can be used in a more metaphorical sense to describe the weeks following delivery

{kind=link}